
Day 2 :
Keynote Forum
Pieter A. Doevendans
University Medical Center Utrecht, The Netherlands
Keynote: Efficacy of renal denervation in the porcine Model
Time : 10:00-10:40

Biography:
Pieter Doevendans became a cardiologist in Maastricht. In 1993-1994 he had the opportunity to work with Ken Chien at UCSD San Diego where the work on stem cells started. The work was completed in Maastricht and provided the basis for a thesis on the promoter of the atrialMLC gene. Upon return in the Netherlands he worked with Christine Mummery and Hans Clevers (Hubrecht Laboratory). In the meantime he remained active as an interventional cardiologist initially in Maastricht, but from 2002 on in Utrecht. Here he was appointed full professor in Cardiology in 2004 and head of the department in 2005. He was funded by various national and international foundations.
Abstract:
Rationale: Recently, the efficacy of renal denervation (RDN) has been questioned. It is discussed whether RDN is able to adequately reach the renal nerves.
Objective: We aimed to investigate how effective RDN was by means of functional hemodynamic measurements and nerve damage on histology.
Methods and results: We performed hemodynamic measurements in both renal arteries of healthy pigs using a Doppler flow and pressure wire. Subsequently unilateral denervation was performed, followed by repeated bilateral hemodynamic measurements. Pigs were terminated directly after RDN or were followed for 3 weeks or 3 months after the procedure. After termination, both treated and control arteries were prepared for histology to evaluate vascular damage and nerve damage. Directly after RDN, resting renal blood flow tended to increase. In contrast, renal resistance reserve increased significantly during follow-up. Vascular histopathology showed that most nerves around the treated arteries were located outside the lesion areas, whereas only14% of the nerves per pig were observed within a lesion area. Subsequently, a correlation was noted between a more impaired adventitia and a reduction in renal resistance reserve (β: -0.33; P=0.05) at three weeks of follow-up
Conclusion: Only a small minority of renal nerves was targeted after RDN. Furthermore, more severe adventitial damage was related to a reduction in renal resistance in the treated arteries at follow-up. These hemodynamic and histological observations may indicate that RDN did not sufficiently target the renal nerves. Potentially, this may explain the significant spread in the response after RDN.
Figure 6: Title: Nerve damage outside the lesion area Legend: 3 weeks histology results showing a treated vessel with nerve damage outside the lesion area. A 20 x magnification (a-e) zooms in on the affected nerve that is indicated with an arrow in picture 1- 6. Serial sections were stained with HE, MST, α-SMA, S100, PGP9.5 and TH. The perineurial tissue and nerves located at the opposite site of the lesion were affected by an extensive inflammatory 21 response (1,a and 2,b), increased proliferation of myofibroblasts (3,c), a reduction in neural tissue (4,d;5,e) and loss of neurotransmitter production of the affected nerves. (adapted from publication in PlosOne 2015).
Keynote Forum
Attila Kardos
Milton Keynes University Hospital, UK
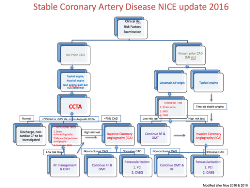
Keynote: What is new in the assessment of patients with chest pain ESC and the NICE recommendations
Time : 10:00-10:50

Biography:
Attila Kardos is a consultant cardiologist at Milton Keynes University Hospital NHS Foundation Trust and a Hon Senior Lecturer to the Division of Cardiovascular Medicine, Radcliffe Department of Medicine Oxford University. He is a clinical lead in multimodality Cardiovascular Imaging and a Director of Research and Development of the Trust. His research interest includes advanced imaging based recognition or cardiovascular pathologies utilizing Cardiac MRI , Cardiac CTA, and advanced echocardiography. His earlier research encompasses exercise physiology and the influence of the autonomic nervous system on exercise performance. Dr Kardos is Chief investigator on in the VECTRA CEB research project that investigates the utility of electrical biomarker in chest pain assessment. He has been and currently is a local principle investigator in several multi-centric trials e.g. EMPHESIS, PARADIGME, PARADIGME –Extent, IMPROVE-IT, RAPID –CTCA, EVAREST, EUROASPIRE-V, SUPPORT-HF2. He is also a member of several Editorial board of a variety of scientific journals.
Abstract:
The prevalence of chest pain presentation to the emergency department is in the range of 25-30%. Stable coronary artery disease has a relatively good long-term outcome with low MCAE rate. The standardization of the diagnosis and management of chest pain patients had been proposed by the European Society of Cardiology and the UK National Institute of Health and Care Excellence (NICE) in 2013 and 2010 respectively. The evolution of diagnostic modalities in cardiology and the evidence from imaging based RCT the triple pillars of chest pain diagnostics (clinical symptoms and risk factors, pre-test probability assessment, and a variety of diagnostic tests for risk stratification) as has been simplified to symptomatic assessment and anatomical imaging of coronary arteries by Cardiac CT Angiography as a gate keeper modality in the update documents of the NICE guidelines in November 2016. Utilizing its high negative predictive accuracy CCTA can be used as a rule out test but equally can predict event depending on the extent and severity of coronary artery disease. Functional test like stress echocardiography, myocardial nuclear perfusion scintigraphy, CMR perfusion have a different role in detecting objective sign of ischaemia in patients with equivocal or moderate degree of coronary artery stenosis on CCTA and in patients with previous coronary artery disease who present with uncertain chest pain symptoms. Those patients only who had sever coronary stenosis on CCTA or present with typical chest pain with prior know CAD will be considered for invasive coronary angiography with view to risk stratify/deliver treatment. In this talk the currently operational guidelines will be reviewed and discussed.
References:
- Eur Heart J 2013;34:2949–3003 - doi:10.1093/eurheartj/eht296
- Chest pain of recent onset. Assessment and diagnosis. November 2016 NICE
- Sessions
Location: Amsterdam, Netherlands
Session Introduction
Soha M. Abd El Dayem
National Research Centre, Egypt
Title: Relationship of nitric oxide genotype to diabetic nephropathy and atherosclerosis of type 1 diabetic patients
Time : 11:05-11:35

Biography:
Soha Abd El Dayem is working in the Medical Service Unit in National Research Center as a Consultant of Diabetes and Endocrinology. She is also working in
Health Insurance as a Consultant of Diabetes and Endocrinology. She is a consultant of Pediatrics in Suzan Moubarak Hospital. She is the member of Society of Egyptian Society of Cardiology.
Abstract:
Objective: Assessment of nitric oxide genotype in diabetic patients and to evaluate its relationship to diabetic nephropathy and atherosclerosis of type 1 diabetic patients.
Patients and methods: The study included 65 type 1 diabetic patients and 30 age and sex matched healthy volunteers. The mean age of patients was 17.99 ± 2.59, mean duration of diabetes was 10.91 ± 3.54, mean onset of disease was 7.00 ± 3.28. Blood samples were taken for assessment of glycosylated hemoglobin (HbA1), lipid profile, oxidized low-density lipoprotein (OxLDL) and serum level of nitric oxide by enzyme linked immunosorbent assay (ELISA) technique. Also, nitric oxide genotype was done. Urine samples were taken for assessment of albumin/creatinine ratio. Carotid intima-media thickness (cIMT) and renal dopplar via ultrasound were also done.
Results: Nitric oxide was significantly lower, while lipid profile, OxLDL and albumin/creatinine ratio, cIMT and resistivity index were significantly higher in diabetic patients. No significant difference of nitric oxide genotype was found in diabetics and control. Nitric oxide was significantly lower, while OxLDL, albumin/ creatinine ratio and lipid profile were significantly higher in nitric oxide homozygous genotype. Conclusion: diabetic patients had a low level of nitric oxide and early atherosclerosis. Nitric oxide homozygous genotype is associated with diabetic nephropathy and atherosclerosis.
Ahmed A. Battah
Cairo University, Egypt
Title: Apelin, nitric oxide and vascular affection in adolescent type 1 diabetic patients
Time : 11:35-12:05

Biography:
Ahmed Abdelrahman Battah is a Professor of Critical Care Cardiology Cairo University. He is working as Interventional Cardiology & Echocardiography Consultant at Cairo University hospitals & Al Salam International Hospital. He is also the member of the European society of Cardiology, Member of the European Critical Care, Member of the Egyptian Society of Critical Care Medicine, Member of the Egyptian Society of Cardiology.
Abstract:
Objective : We are aiming to evaluate apelin and nitric oxide (NO) in type 1 diabetic patients and its relation to vascular affection.
Patients and methods: The study included 62 type 1 diabetic patients and 30 healthy volunteers of the same age and sex. Blood samples were taken for assessment of apelin, NO, glycosylated hemoglobin, and lipid profile. Urine samples were taken for assessment of albumin/creatinine ratio flow mediated dilatation (FMD) via ultrasound was done .
Results: The mean age of diabetic patients were 16.3 ± 1.5 yrs ( 14.0 – 19.0 yrs), and mean duration of diabetes were 9.4 ± 2.9 yrs ( 5.0 – 16.5 yrs). FMD and FMD/ nitrate mediated dilatation (NMD) ratio were significantly lower in diabetics. Nitric oxide was significantly lower , while apelin and albumin/ creatinine ratio were significantly higher than controls. No significant correlation was found between apelin, NO, FMD, albumin / creatinie ratio or BMI.
Conclusion: Diabetic patients had endothelial dysfunction and elevation of apelin, but they does not related to each other. BMI had no relation to apelin which indicate that obesity had no role to apelin. Further large study is recommended to detect the relationship of apelin with vascular affection by assesseing large numer of diabetics with and without complication.
Alan Fleming
Optos, Dunfermline, UK
Title: A proposed study in detection of hypertension by ultra-widefield ophthalmic imaging
Time : 12:05-12:35

Biography:
The authors have many years experience in developing algorithms for retinal image analysis in industry and academia. Alan Fleming has many publications in this field from University of Aberdeen. Gavin Robertson completed his PhD at University of Edinburgh in retinal vascular analysis. Jano van Hemert has led multidisciplinary research groups in academia and industry and is an ardent exponent in the commercialisation of research output.
Abstract:
Statement of the Problem: Ophthalmic imaging may provide a method for hypertension detection. Changes to the caliber of the retinal vasculature near the optic disc are early biomarkers of hypertension. We hypothesize that changes in vessel caliber in ultra-widefield scanning laser ophthalmoscope (UWF-SLO) images can be used to classify hypertensive status. A pilot study with 500 subjects has shown that software (optomapHT, Optos, UK) for semi-automated detection of venular and arteriolar caliber in UWF-SLO images can predict hypertensive status, defined by clinical blood pressure (BP) >= 140mmHG, area under receiver operator characteristics curve (AUROC) of 0.720.
Proposed study aim: To determine the ability of optomapHT to predict hypertensive status as established through either ambulatory BP measurement or clinical BP measurement.
Study design: Ambulatory BP measurements provide a better prediction of retinal arteriole caliber than clinical BP. However, the procedure for ambulatory BP measurement may cause discomfort for the patient making population based studies difficult.Therefore, the proposed study participants will be patients whose routine care includes either ambulatory BP or clinical BP measurement. Informed consent will include agreement to undertake, in addition, UWF-SLO retinal imaging. Outcome measures will be AUROC for the prediction by optomapHT of hypertension according to clinical BP or ambulatory BP. To show that optomapHT is at least equivalent to clinical BP for diagnosis of hypertensive status 600 participants are required,.
Conclusion: In addition to eye care, UWF-SLO imaging technology presents an opportunity for early detection of hypertensive patients. Collaborators in this study would benefit from partnership with a highly successful ophthalmic imaging company.
Ahmed A. Battah
Cairo University, Egypt
Title: Glycemic control and carotid intimal medial thickness in adolescents type 1 diabetic patients : a three years follow up
Time : 12:35-13:05

Biography:
Abstract:
Objective: To assess carotid intimal medial thickness(cIMT) in type 1 diabetic patients who were followed up for 3 years to shed further light on relationship of glycemic control and cIMT.
Patients and methods: It is a prospective cohort observational study, included 40 type 1 diabetic patients and 30 age and sex matched healthy volunteer. Blood sample was taken for analysis of glycosylated hemoglobin (HbA1), lipid profile and urine sample was taken for analysis of albumin/ creatinine ratio. cIMT via ultrasound was also done. Three years later, patients were subjected to the original laboratory investigation and cIMT. t- test and MacNemar test was used for analysis of data.
Results : cIMT were significantly higher in diabetics in the original study. Three years later, patients had significant increase in waist/ hip ratio, HbA1, albumin/ creatinine ratio and cIMT. cIMT regressed in 3 patients, remained stationary in 18 patients (2 patients remain normal and 16 had increased cIMT) and the remaining 19 patients had progressed cIMT. Patients with progressed cIMT had significantly higher waist/ hip ratio, HbA1and albumin/ creatinine ratio than patients with stationary cIMT.
Conclusion: Adolescent type 1 diabetic patients had increased cIMT. Progression in cIMT is associated with obesity, poor glycemic control and nephropathy. We recommend good glycemic control and frequent follow up of diabetic patients for early detection of diabetic complication.
Soha M. Abd El Dayem
National Research Centre, Egypt
Title: Relationship of plasma level of nesfatin, chemerin and vaspin to early atherosclerotic changes and its genetic study in adolescent type 1 diabetic patients
Time : 13:05-13:35

Biography:
Soha Abd El Dayem is working in the Medical Service Unit in National Research Center as a Consultant of Diabetes and Endocrinology. She is also working in
Health Insurance as a Consultant of Diabetes and Endocrinology. She is a consultant of Pediatrics in Suzan Moubarak Hospital. She is the member of Society of Egyptian Society of Cardiology.
Abstract:
Objective: To evaluate the relationship of plasma level of nesfatin, chemerin and vaspin to early atherosclerotic changes. Also to evaluate chemerin and vaspin genotype and to detect its relation to glycemic control and atherosclerosis in adolescent type 1 diabetic patients.
Patients and methods: The study included 70 type 1 diabetic patients and 30 age and sex matched healthy volunteers. The mean age of patients was 17.99 ± 2.59, mean duration of diabetes was 10.91 ± 3.54, mean onset of disease was 7.00 ± 3.28. Blood samples were taken for assessment of chemerin, nesfatin, vaspin, and oxidized low-density lipoprotein (OxLDL) by enzyme linked immunosorbent assay (ELISA) technique. Also, blood samples were taken for analysis of glycosylated hemoglobin (HbA1); lipid profiles and urine samples were taken for assessment of albumin/creatinine ratio. Carotid (cIMT) and aortic (AIMT) intima-media thickness were also done.
Results: Nesfatin, chemerin, vaspin, OxLDL, albumin/creatinine ratio, cIMT and AIMT were significantly higher in diabetic patients. HbA1 and cIMT were significantly higher in homozygous (TT) genotype of chemerin than GG genotype (9.50 ± 1.99 vs 8.34 ± 1.62 and 0.54 ± 0.06 vs 0.50 ± 0.04 respectivelly). Chemerin and vaspin had a significant positive correlation (r = 0.2, P = 0.05), nesfatin and LDL (r = 0.3, P = 0.05) and Vaspin and body mass index (r = 0.3, P = 0.01).
Conclusion: Diabetic patients had increased level of adipocytokines and are liable for early atherosclerosis. Homozygous genotype (TT) of chemerin in diabetic patients is associated with poor glycemic control and early atherosclerosis.
- Workshop
Location: Amsterdam, Netherlands
Session Introduction
Louis Peeters
Utrecht University, Netherlands
Title: Pathophysiology of Hypertensive Disorders of Pregnancy (HDPs): Current insights

Biography:
Louis Peeters dedicated most of his scientific career to the study of maternal physiology in pregnancy and of the pathophysiology of hyperten- sive pregnancy disorders, both in animals and women. He started his career in 1974 with a fellowship in Fetal & Maternal Medicine at the Un. of Colorado, Denver. After his residency in Ob/Gyn. (1976-1981, Nijmegen, the Netherlands), he worked at the Dept. of Ob/Gyn., Erasmus Univ., Rotterdam and from 1987 at the Dept of Ob/Gyn, MUMC, Maastricht. In 1987 and 2001/2002, resp., he interrupted his work in the Netherlands for sabbaticals at Columbia Univ, New York City (Dept. Physiology) and UCSF, San Francisco (Dept. Ob/Gyn.). From 2011 he worked at the Dept. Ob., UMC Utrecht, to retire from clinical duties in 2013. Afterwards he continued his work in education and research. During his career he published over 150 scientific articles and over 20 book chapters.
Abstract:
Introduction: Current management of HDPs is symptomatic intended to 1) prevent deterioration of unstable cardiovascular and renal functions, and 2) minimize the infant’s risk of permanent hypoxia/prematurity- related damage. Since ≈1980 our insight in the normal and abnormal cardiovascular and volume responses to normal and HDP-pregnancies has improved markedly, offering options to develop more causal and with it, probably more effective HDP management strategies.This lecture summarizes current insights in the mechanisms orchestrating maternal cardiovascular/volume responses to pregnancy, and with it, provides clues when and how these normal adaptations deteriorate allowing HDP to develop.
Normal cardiovascular adaptation: Within 10 days after embryo im- plantation, plasma osmolality (fig. 1) and arterial blood pressure [2] fall abruptly, probably echoing the hemodynamic effects of systemic vascular relaxation and associated fall in cardiac pre- and afterload. They trigger adaptations, which serve to secure circulatory functional integrity. Cardiac preload is restored by endocrine-induced plasma volume expansion along with the concomitant development of a more negative intrathoracic (suction) pressure. Cardiac afterload is restored by a rise in cardiac output (CO) via a baroreceptor-mediated rise in cardiovascular sympathetic tone. Preservation of the balance between cardiac pre- and afterload is pivotal for optimal cardiac function all through pregnancy (3, 4, 5).
Defective cardiovascular adaptation: Inherent to HDPs being defined by clinical signs is the heterogeneity of its preclinical pathophysiologic course. Nowadays, it is customary to differentiate between early- and late-onset HDP, primarily as they require a different clinical manage- ment. As a rule of thumb, physiologic adaptation to pregnancy deterio- rates when the balance between cardiac pre- and afterload becomes disturbed, necessitating a higher sympathetic contribution to the auto- nomic regulation of the circulatory function to preserve cardiovascular functional integrity, though, at the cost of the uteroplacental perfusion and with it, the growth of the placental functional capacity.
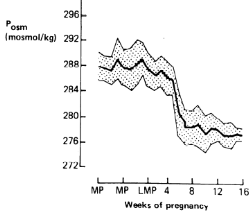
Figure 1: Weekly plasma osmolality (Posmol ± SD) before and during early pregnancy in 9 healthy pregnancies. MP and LMP indicate menstrual and last menstrual periods, respectively. (Adopted and modified from ref 1).
References:
- Davison JM et al, Plasma osmolality and urinary concentration and dilution during/after pregnancy. Brit J Obstet Gynaecol 1981;88:472.
- Spaanderman ME et al, The effect of pregnancy on the compliance of large arteries and veins in normal parous controls and formerly preeclamptics. Am J Obstet Gynecol 2000; 183: 1278.
- Valdes G et al. Challenges posed to the maternal circulation by preg- nancy (review). Integrated Blood Pressure Control 2011; 4: 45.
- Melchiorre K et al. Cardiac structure & function in normal pregnancy.Curr. Opin. Obstet. Gynaecol. 2012; 24: 413.
- Melchiorre K et al. Cardiac structure & function in normal pregnancy.Curr. Opin. Obstet. Gynaecol. 2012; 24: 413.Chung E et al. Pregnancy as a cardiac stress model. Cardiovasc. Res. 2014; 101: 561-570.
Marc Spaanderman
Maastricht University , Netherlands
Title: Risk group identification, prevention and early detection of Hypertensive Disorders of Pregnancy (HDP)

Biography:
Marc Spaanderman, MD PhD, is chair of the department of Obstetrics Maastricht University Medical Center MUMC. The past 20 years, his research group focusses on maternal health and the capacity to balance cardiovascular stress before, during and after pregnancy. As expertise center, his department structures its care around this topic in order to personalize treatment in an attempt to prevent future health problems during pregnancy and thereafter. Ways to improve patient empowerment and participation in individuals’ care are central themes in the departments’ health promoting programs. As initiator and president of the Limburg Obstetric Consortium, an obstetric-midwifery-maternity care and neonatology collaboration, he stands for structured and uniformly supplied transparent care for pregnant women and thereafter.
Abstract:
Statement of the problem: Vascular complications may arise from pre-existing cardiovascular risk factors that lower the capability to withhold the increased hemodynamic mechanical and biochemical burden of gestation or from reduced physiological adaptive capability during the first half of gestation. Although the biological diversity in jeopardizing actions of associate risk factors implies tailored preventive measures, so far, most developed preventive strategies are rather generic than specific. Systematic risk analysis of those having encountered vascular complications throughout gestation may shed light on underlying dis-orders and with it tailored preventive strategies (Fig 1). Moreover, early-pregnancy maternal adaptive responses may additionally identify those at increased risk.
Methodology and theoretical orientation: Prior to pregnancy, short sys-tematic evaluation of associated risk factors consistent with the metabolic syndrome and larger evaluation in those with prior vascular complicated pregnancy or preexisting disease associated with gestational vascular disorders may detect those at increased risk. Circulatory follow-up throughout the first half of gestation could be helpful in detecting those failing to circulatory adjust properly, increasing their risk additionally.
Findings: Generic preventive measures, such as aspirin and calcium, should be discussed in those with anticipated increased risk. Precision medication should be offered to those with serious underlying disorders as SLE and antiphospholipid syndrome, kidney disease, prior thrombotic events, chronic hypertension or cardiac failure. In order to improve maternal outcome, antihypertensive drugs should be instituted at the level of mild to moderate hypertension throughout gestation.
Conclusion and significance: Vascular complications in pregnancy may arise from preexisting cardiovascular, cardio-metabolic, hemostatic or autoimmunological risk factors. Besides generic preventive actions, precision measures can be discussed and taken depending on personal underlying disorders.
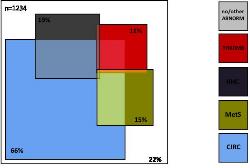
Figure 1; underlying hemodynamic, metabolic and hemostatic risk factors in 1234 non-pregnant formerly preeclampic women. (Adapted and modi-fied from reference 1)
References:
- Scholten R et al. Co-occurrence of cardiovascular and prothrombotic risk factors in women with a history of preeclampsia. Obstet Gynecol. 2013 Jan;121(1):97-105.
- Roberge S et al. The role of aspirin dose on the prevention of pre-eclampsia and fetal growth restriction: systematic review and meta-analysis. Am J Obstet Gynecol. 2016: S0002-9378(16) 30783-9.
- Hofmeyr G et al. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev. 2014 Jun 24;(6):CD001059.
- Abalos E et al. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev. 2014 Feb6;(2): CD002252.
- Magee L et al. Less-tight versus tight control of hypertension in preg-nancy. N Engl J Med. 2015 Jan 29;372(5):407-17.
Johannes J. (Hans) Duvekot
Erasmus University, Netherlands
Title: Current management of Hypertensive Disorders of Pregnancy (HDPs)
 Duvekot")
Biography:
Johannes J. (Hans) Duvekot is a consultant in obstetrics and perinatology at the Erasmus MC, University Medical Center in Rotterdam, the Netherlands. In his clinical career, which started in 1984, he dedicated himself to the study of maternal hemodynamics and related disturbances like preeclampsia. During his residency at the University Hospital of Maastricht, he wrote his thesis on early changes in maternal hemodynamics and volume homeostasis. He participated in the Magpie trial that formed a milestone in prevention of eclampsia. Since 2003 he is working at the Erasmus MC in Rotterdam, where he is involved in clinical studies on preeclampsia and the long-term effects of this disease on women. He published over 150 scientific articles and over 15 book chapters.
Abstract:
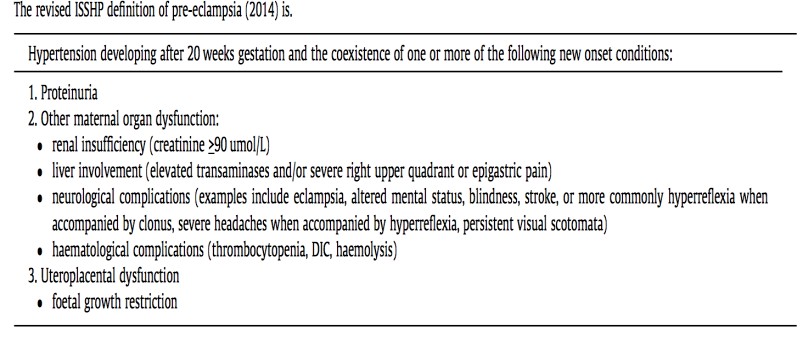
Introduction: Between 2 and 8% of pregnancies are complicated by preeclampsia (PE) defined as specified in table 1(1). At present, the only ultimate “cure” of PE and other forms of HDPs is removal of the placenta and thus, delivery. As the clinician provides “combined care” to 2 risk patients, treatment focuses on prevention of both maternal and fetal morbidity. In ≈1/3 of cases the dilemma arises that the prematurity risk outweighs maternal risks of ongoing HDP pregnancy. In ≈2/3 of cases, HDP symptoms develop >36 weeks with acceptable prematurity risks for the infant. However, at this later gestational age maternal risks are not lower! Most maternal deaths occur in the last half of pregnancy, even though the incidence of maternal death is 20-fold higher in early- onset PE. The latter is related to the much higher incidence of severe disease in early-onset PE. In developed countries PE accounts for ≈19% of maternal deaths (2).
Acute treatment: Severe HDP ought to be treated by a multidisciplinary team (obstetrician, neonatologist, and anesthesiologist). Initially, prompt stabilization by controlling blood pressure along with MgSO4 admini- stration to prevent eclampsia is of utmost importance. In most cases intra- venous administration of antihypertensives is needed. After reaching a clinically stable maternal condition, the clinician has to decide how and when to deliver the infant (2).
Temporizing management or not: In severe HDP temporizing management is only recommended after the 24th week. The best management of severe HDP between 28 and 34 weeks is still open to debate. After 34 weeks it is generally accepted to deliver women with severe HDP shortly after maternal stabilization. Between 34 and 37 weeks, temporizing management of mild HDP may be especially beneficial for the fetus (3). After 37 weeks induction of labor or elective cesarean section is strongly recommended (4). In the decision whether or not to prolong pregnancy, evaluation by a risk score may help to decide. The so-called “full-Piers” model gives some important clues for pending morbidity (5).
Table 1 (adopted from ref 1).
References:
- Tranquilli A et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens 2014; 4: 97.
- Steegers E et al. Pre-eclampsia. Lancet 2010; 376: 631.
- Broekhuijsen K et al (HYPITAT-II study group). Immediate delivery versus expectant monitoring for hypertensive disorders of pregnancy between 34 and 37 weeks of gestation (HYPITAT-II): an open-label randomized controlled trial. Lancet 2015; 385: 2492.
- Koopmans C et al. (HYPITAT study group). Induction of labour versus expectant monitoring for gestational hypertension or mild pre- eclampsia after 36 weeks' gestation (HYPITAT): a multicentre, open- label randomised controlled trial. Lancet 2009; 374: 979.
- von Dadelszen P et al. (PIERS Study Group.. Prediction of adverse maternal outcomes in pre-eclampsia: development and validation of the full PIERS model. Lancet 2011; 377: 219.
Peter de Leeuw
Maastricht University , Netherlands
Title: Options for novel, pathophysiology-based management of Hypertensive Disorders of Pregnancy (HDPs)

Biography:
Peter de Leeuw is emeritus professor of Medicine at the Maastricht University Medical Center. His clinical and research interest goes to vascular me-dicine with particular reference to hypertension and related disorders. He has published over 700 papers on hemodynamics, neurohumoral abnor-malities and drug treatment in hypertension. Most recently, he has been involved with baroreceptor stimulation as a novel treatment of resistant hy-pertension. He has been President of the Dutch Hypertension Society and a Council Member of the International Society of Hypertension. Moreover, he has been Editor-in-Chief of three medical journals in internal medicine.
Abstract:
Introduction: From a hemodynamic point of view, hypertension may be caused by an increase in cardiac output and/or peripheral vascular resistance. In addition, volume status and the degree of vascular stiffness determine the height of blood pressure. When hypertension is found during pregnancy (HDPs), all these pathophysiological phenomena may play a role but the pattern is far from homogeneous. First, it makes a difference whether hypertension was pre-existent or induced by the pregnancy. Secondly, it is important to consider that HDP may involve as a spontaneous disorder in an otherwise healthy woman or be superimposed upon another ‘silent’ underlying abnormality.
Pathophysiological considerations: In pregnancy-related hypertension we usually find a lower cardiac output, increased vascular resistance, increased arterial stiffness and a reduced plasma volume. The activity of the renin-angiotensin system is suppressed as well. This suggests that there is a hypertensive stimulus which leads to a compensatory reduction in pressor systems. The fact that sympathetic activity is activated rather than suppressed can be seen as an attempt to ‘keep the circulation going’.
Pathophysiology-based management:The most appropriate approach to the patient with a HDP is to direct treatment to those factors that could initiate or exacerbate a rise in pressure. Recent evidence suggests that a substantial proportion of women with preeclampsia - a common form of HDP - have renal vascular abnormalities, either as a pattern of intrarenal nephrosclerosis or, and perhaps more often, as macrovascular disease, notably fibromuscular dysplasia.
References:
- Vance CJ et al. Increased prevalence of preeclampsia among wo-men undergoing procedural intervention for renal artery fibro-muscular dysplasia. Ann Vasc Surg 2015; 29: 1105.
- Spaanderman ME et al, The effect of pregnancy on the compliance of large arteries and veins in normal parous controls and formerly preeclamptics. Am J Obstet Gynecol 2000; 183: 1278.
- Abalos E et al. Antihypertensive drug therapy for mild to mode-rate hypertension during pregnancy. Cochrane Database Syst Rev. 2014 Feb6;(2): CD002252.
- Van Twist DJ et al. Renal hemodynamics and renin-angiotensin sys-tem activity in humans with multifocal renal artery fibromuscular dysplasia. J Hypertens 2016; 34: 1160.
- De Leeuw PW et al. Bilateral or unilateral stimulation for baroreflex activation therapy. Hypertension 2015; 65: 187.
- Posters
Location: Amsterdam, Netherlands
Session Introduction
Hsuan Lo
Tzu University, Taiwan
Title: Altered NMDA receptor-nitric oxide (NO) signaling in the rostral ventrolateral medulla contribute to cardiovascular response of acute ethanol-exposure

Biography:
Hsuan Lo is a PhD scholar, studied in the Department of Pharmacology and Toxicology at Tzu Chi University. His lab is interested in neuropharmacology particularly in alcohol effects on the central nervous system and cardiovascular function. His studies focus on the mechanism of acute ethanol intake action on the glutamate signaling within the rostral ventral lateral medulla (RVLM). He has performed the whole animal model with practiced skill in RVLM, microinjection of drug and femoral artery surgery for measuring blood pressure, and also have set up the HPLC system to detect the neurotransmitter content. On the other hand, his master's thesis was of Amyloid-beta peptides on NMDA receptor activation in rat sympathetic preganglionic neurons using whole cell, patch clamp technique. All his training has led him to know more about, how the CNS works to control cardiovascular function.
Abstract:
Consumption of ethanol (EtOH) has many effects on physiological functions particular in the central nerve system and cardiovascular system. Hypotension is one of the main features of acute excessive intake of ethanol (alcohol intoxication). In addition, chronic ethanol consumption has been associated with cardiovascular diseases, including hypertension and stroke. The precise mechanisms underlying ethanol regulation of cardiovascular function remains unclear. It is well known that central N-Methyl-D-Aspartate (NMDA) receptors are implicated in the modulation of glutamatergic transmission and important in regulating neuronal activity. Recent evidence also suggests that nitric oxide is a key neuromodulator within the central nervous system and its production is associated with NMDA receptor activation. The rostral ventrolateral medulla (RVLM) is known as a vasomotor center, which provides the basal sympathetic outflow and maintains blood pressure (BP). This study was carried out to test the hypothesis that NMDA and NO signaling in the RVLM are involved in the regulation of ethanol-induced changes in BP. The BP response was measured in urethane anesthetized SD rats weighing 280-350 g. EtOH (3.2 g/kg) was applied by intraperitoneal injection (IP). The samples of glutamate and NO were collected by micro dialysis every 15 minutes in the RVLM and then analyzed with HPLC-ECD and NOx analyzer, respectively. The results showed that IP ethanol elicited a significant increase in the level of glutamate and NO in RVLM and a reduction in BP. Microinjection of ketamine (an NMDA receptor antagonist) or L-NNA (an NOS inhibitor) into the RVLM, which was applied 5 min after administration of EtOH, attenuated EtOH-induced depressor effects. In addition, microinjection of ketamine suppressed the level of NO production. The results suggest that increases in NMDA receptors activation and enhancement of NO synthase activity in the RVLM may play a major role in ethanol-evoked hypotension.